
RECHERCHE ET DEVELOPPEMENT
Mes activités de recherche expérimentale ont porté notamment sur les matériaux prothétiques, sur les transplantations et sur le développement d'instruments chirurgicaux.
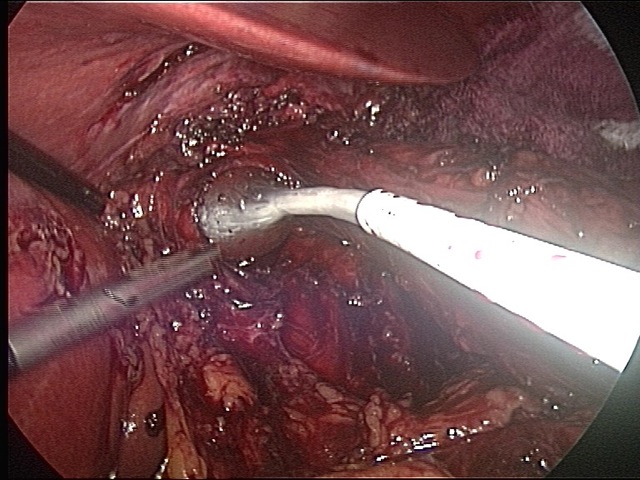
Ici un exemple d'un instrument original pour calibrer le hiatus oesophagien au cours de la cure laparoscopique d'un reflux gastro oesophagien.
G. Fourtanier
A new method to calibrate the hiatus
Surgical Endoscopy 2007, 21, 1674
Reardon in his letter to the editor discussed the hiatus closure during laparoscopic total fundoplication (1). As Granderath et al reported in a recent article (2), this is in fact a crucial point of the technique to avoid postoperative dysphagia as well as intrathoracic migration of the wrap.
The problem that Reardon explains well in his letter is to know how tightly the crura should be closed and to find an objective way to do it. As related in his letter, he, himself, just starting to perform laparoscopic 360° fundoplication and repairs of hiatal hernia, was immensely frustrated when he listening to lectures of experts or when he asked them exactly how they closed the crura, because of the vague, subjective answers, to the question of the precise details as to how tight to close the crura.
His proposal, qualified as “modest”, but really contributive, is based on the intraoperative measurement of the hiatus before and after closure. We agree with him that the diameter of the hiatus should be measured anteroposteriorly according to the same landmarks, from the most anterior point of the hiatus, to the point at which the left crus and right crus join posteriorly. In our experience, we also measure the largest distance between the both cruras. For both measurements we use a tape measured outside the abdomen once the precise distances of the anatomic structures have been landmarked inside. These data are recorded in the operative report and can be useful to compare the procedures especially if a trial is planned.
Reardon states that the appropriate final anteroposterior diameter for the closure of the hiatus is 18 to 20mm over a 60-Fr bougie, leaving an adequate room for passage of a food bolus. Nevertheless in his opinion, studies would be required to compare this “ideal diameter” with the results of others in order to find the “ideal” tradeoff between preventing intrathoracic migration and postoperative dysphagia..
We agree that, the closure of the hiatus is an important step of an antireflux surgery and that calibration seems essential: it should be reproducible for all surgeons.
Through laparotomy, we used to do that by placing a finger between the esophagus and the closure of the hiatus. We tried to reproduce the maneuver through laparoscopy by placing a Fogarty or a Foley catheter, passed through a 10mm trocar, inflated with 4ml of serum, in order to obtain the same diameter as a finger. In a personal series comparing 21 partial wraps with calibration of the hiatus to 21 cases in which the hiatus was not calibrated (3), we found that dysphagia at 2 months postoperatively was frequent (66% vs. 48%, difference NS) but with a statistically shorter duration of dysphagia thanks to the calibration (25days vs. 43days p<0.05).
Recently, we have developed an instrument to calibrate the hiatus named HiaTech® (Laboratoire Surgical IOC Saint Etienne France). The disposable instrument, 40 cm long and rigid is passed through a 5mm trocar. At the tip of the HiaTech®, a silicone balloon inflated with 9ml of serum will reproduce a finger shape 30mm long and 12mm large. This maneuver is quick, safe, and easily reproducible for every surgeon. A prospective multicenter trial including 120 patients (9 European centers) is now underway to compare the outcome (on one hand the frequency and the severity of eventual dysphagia and on the other hand, the prevention of intrathoracic migration of the wrap), comparing two groups of patients with or without calibration by HiaTech®.
References
1. Reardon PR (2006) A modest proposal. Surg Endosc 20: 995
2. Granderath FA, SchweigerUM, Kamolz T, Pointner R (2005) Dysphagia after laparoscopic antireflux surgery : a problem of hiatal closure more than a problem of the wrap. Surg Endosc 19: 1439-1446
3. Sledzianowski JF, Suc B, Lizza N, Muscari F, Gahnnem Y, Duffas JP, Fourtanier G (2002) Le calibrage de l’orifice hiatal diminue la dysphagie post-opératoire après la cure de reflux gastro-oesophagien par laparoscopie : étude cas-témoins. Ann Chir 127 :175-180